Get Tennessee First Report Template in PDF
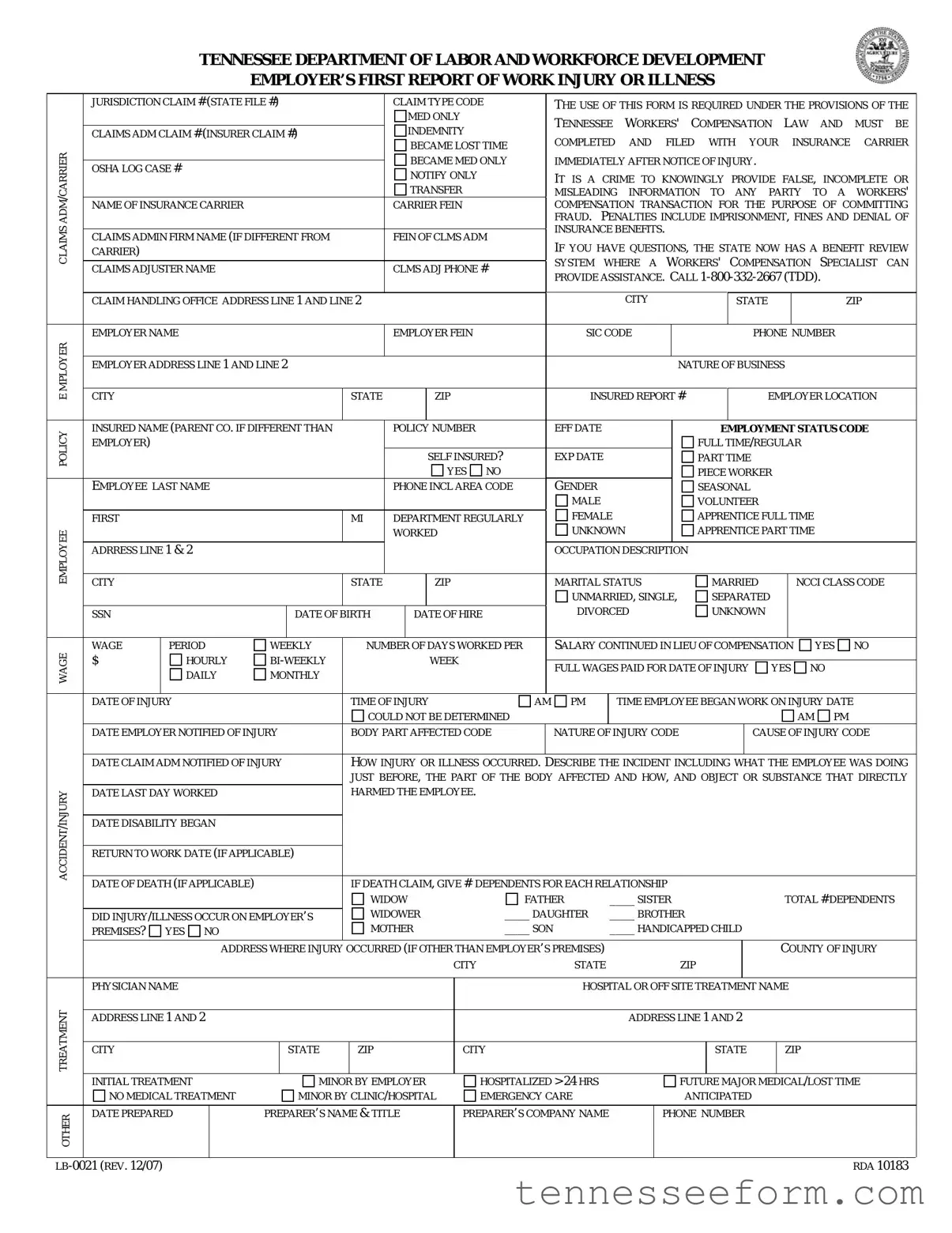
In the realm of worker's compensation within Tennessee, the Employer's First Report of Work Injury or Illness plays a pivotal role. Mandated by the Tennessee Workers' Compensation Law, this detailed document, known formally under the designation LB-0021 (Rev. 12/07) RDA 10183, requires completion and submission to the employer's insurance carrier promptly after an injury or illness occurs at the workplace. It includes a comprehensive array of information such as jurisdiction claim number, type of claim, details about the insurance carrier, the employer, and the injured or ill employee. Crucially, the form serves to document the nature and circumstances of the incident, including specifics about the injury or illness, the affected body part, and the initial treatment provided. Moreover, it features fields for documenting the injury's impact on the employee's work status, including time of injury, last day worked, and the anticipated return to work. The form also outlines the legal ramifications for knowingly providing false information, emphasizing the seriousness of the submission in combating fraud and ensuring that the claims process proceeds with integrity. It represents a critical first step in the claims process, aiming to facilitate a swift and fair resolution for employees suffering from work-related injuries or illnesses..
Document Preview Example
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
EMPLOYER’S FIRST REPORT OF WORK INJURY OR ILLNESS
|
JURISDICTION CLAIM # (STATE FILE #) |
|
|
|
CLAIM TYPE CODE |
|
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
MED ONLY |
|
|
TENNESSEE |
WORKERS' |
|
COMPENSATION |
LAW |
AND |
MUST |
BE |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
INDEMNITY |
|
|
|
|||||||||||||||||||||
|
CLAIMS ADM CLAIM # (INSURER CLAIM #) |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
COMPLETED |
AND |
FILED WITH |
YOUR |
|
|
INSURANCE |
CARRIER |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME LOST TIME |
|
|
|
|||||||||||||||||||||
CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
TRANSFER |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME MED ONLY |
|
IMMEDIATELY AFTER NOTICE OF INJURY. |
|
|
|
|
|
|
||||||||||||||||
|
OSHA LOG CASE # |
|
|
|
|
|
|
|
NOTIFY ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISLEADING INFORMATION TO ANY PARTY TO A WORKERS' |
|||||||||||||||||||
ADM |
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
CARRIER FEIN |
|
|
COMPENSATION TRANSACTION FOR THE PURPOSE OF COMMITTING |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FRAUD. |
PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF |
|||||||||||||||||||
CLAIMS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE BENEFITS. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM |
|
|
|
FEIN OF CLMS ADM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
IF YOU HAVE QUESTIONS, THE STATE NOW HAS A BENEFIT REVIEW |
||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
CARRIER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SYSTEM |
WHERE A |
WORKERS' COMPENSATION |
SPECIALIST |
CAN |
|||||||||||||||
|
CLAIMS ADJUSTER NAME |
|
|
|
|
|
|
CLMS ADJ PHONE # |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
PROVIDE ASSISTANCE. CALL |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CLAIM HANDLING OFFICE ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
ZIP |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
EMPLOYER NAME |
|
|
|
|
|
|
EMPLOYER FEIN |
|
|
SIC CODE |
|
|
|
|
|
|
|
PHONE NUMBER |
|
|
|||||||||||||||
MPLOYERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
INSURED REPORT # |
EMPLOYER LOCATION |
|
|||||||||||||||||||||||
|
EMPLOYER ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
POLICY |
INSURED NAME (PARENT CO. IF DIFFERENT THAN |
|
|
|
POLICY NUMBER |
|
EFF DATE |
|
|
|
|
|
|
EMPLOYMENT STATUS CODE |
|
|||||||||||||||||||||
EMPLOYER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FULL TIME/REGULAR |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF INSURED? |
|
EXP DATE |
|
|
|
|
|
PART TIME |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
GENDER |
|
|
|
|
|
|
|
PIECE WORKER |
|
|
|
|
|
|
||||||
|
EMPLOYEE LAST NAME |
|
|
|
|
|
|
PHONE INCL AREA CODE |
|
|
|
|
|
|
|
|
SEASONAL |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
|
|
|
|
|
|
|
VOLUNTEER |
|
|
|
|
|
|
|||||
|
FIRST |
|
|
|
|
|
|
MI |
|
DEPARTMENT REGULARLY |
|
FEMALE |
|
|
|
|
|
APPRENTICE FULL TIME |
|
|
|
|||||||||||||||
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
WORKED |
|
|
UNKNOWN |
|
|
|
APPRENTICE PART TIME |
|
|
|
|||||||||||||||
ADRRESS LINE 1 & 2 |
|
|
|
|
|
|
|
|
|
|
|
|
OCCUPATION DESCRIPTION |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
MARITAL STATUS |
|
|
|
|
MARRIED |
|
|
NCCI CLASS CODE |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNMARRIED, SINGLE, |
|
|
SEPARATED |
|
|
|
|
|
|
||||||||||
|
SSN |
|
|
|
|
DATE OF BIRTH |
|
|
DATE OF HIRE |
|
DIVORCED |
|
|
|
|
UNKNOWN |
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
WAGE |
|
PERIOD |
WEEKLY |
|
NUMBER OF DAYS WORKED PER |
|
SALARY CONTINUED IN LIEU OF COMPENSATION |
|
YES |
NO |
|
||||||||||||||||||||||||
$ |
|
HOURLY |
|
|
|
|
|
WEEK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
FULL WAGES PAID FOR DATE OF INJURY |
YES NO |
|
|
||||||||||||||||||||||||
|
|
|
DAILY |
MONTHLY |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
DATE OF INJURY |
|
|
|
|
TIME OF INJURY |
|
AM PM |
|
|
TIME EMPLOYEE BEGAN WORK ON INJURY DATE |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
COULD NOT BE DETERMINED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
|
|
||||||
|
DATE EMPLOYER NOTIFIED OF INJURY |
|
BODY PART AFFECTED CODE |
|
NATURE OF INJURY CODE |
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
DATE CLAIM ADM NOTIFIED OF INJURY |
|
HOW INJURY OR ILLNESS OCCURRED. |
DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
JUST BEFORE, THE PART OF THE BODY AFFECTED AND HOW, AND OBJECT OR SUBSTANCE THAT DIRECTLY |
|||||||||||||||||||||||||||
INJURY |
DATE LAST DAY WORKED |
|
|
|
|
HARMED THE EMPLOYEE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ACCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN TO WORK DATE (IF APPLICABLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
IF DEATH CLAIM, GIVE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
DATE OF DEATH (IF APPLICABLE) |
|
|
|
DEPENDENTS FOR EACH RELATIONSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
WIDOW |
|
|
|
FATHER |
|
____ SISTER |
|
|
|
|
|
|
|
TOTAL # DEPENDENTS |
||||||||||||
|
|
|
|
|
|
WIDOWER |
|
|
____ DAUGHTER |
|
____ BROTHER |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
DID INJURY/ILLNESS OCCUR ON EMPLOYER’S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
PREMISES? |
YES NO |
|
|
|
|
|
MOTHER |
|
|
____ SON |
|
____ HANDICAPPED CHILD |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ADDRESS WHERE INJURY |
OCCURRED (IF OTHER THAN EMPLOYER’S PREMISES) |
|
|
|
|
|
|
|
|
|
|
|
COUNTY OF INJURY |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
|
|
|
|
ZIP |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL OR OFF SITE TREATMENT NAME |
|
|
|
|||||||||||||||||||
TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
CITY |
|
|
|
|
STATE |
|
ZIP |
|
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
INITIAL TREATMENT |
|
|
MINOR BY EMPLOYER |
|
|
HOSPITALIZED > 24 HRS |
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/LOST TIME |
|
|||||||||||||||||||||
|
NO MEDICAL TREATMENT |
|
|
MINOR BY CLINIC/HOSPITAL |
EMERGENCY CARE |
|
|
|
|
|
|
ANTICIPATED |
|
|
|
|
|
|
||||||||||||||||||
OTHER |
DATE PREPARED |
|
PREPARER’S NAME & TITLE |
|
PREPARER’S COMPANY NAME |
|
|
PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RDA 10183 |
||||
Document Data
| Fact Number | Fact Detail |
|---|---|
| 1 | The form is required under the Tennessee Workers' Compensation Law. |
| 2 | It must be completed and filed with the insurance carrier immediately after notice of injury. |
| 3 | Providing false or misleading information is a crime that can result in imprisonment, fines, and denial of insurance benefits. |
| 4 | Tennessee has a Benefit Review System for assistance, reachable at 1-800-332-2667 (TDD). |
| 5 | The form captures details about the employer, insurance carrier, and the injured or ill employee. |
| 6 | Specific information about the injury or illness, including how it occurred and the body part affected, is required. |
| 7 | It asks whether the injury or illness resulted in lost time or whether it became a medical-only incident. |
| 8 | Data on the form includes details on the employee's work status, time of injury, and initial treatment received. |
Detailed Guide for Using Tennessee First Report
Filling out the Tennessee First Report form is an important step in the workers' compensation process after an injury or illness occurs at work. This form is essential for documenting the incident and starting the compensation claim. Carefully providing all the requested information ensures that the process goes smoothly and helps to avoid any potential delays or complications. Below are the step-by-step instructions to assist you in completing the form correctly.
- Enter the Jurisdiction Claim # (State File #) and Claim Type Code at the top of the form.
- Fill in the ADM Claim # (Insurer Claim #), noting whether it's a Med Only, Indemnity Claims, or if the status has changed (e.g., Transfer Became Med Only).
- Log the OSHA Log Case # if applicable.
- Write down the Insurance Carrier's Name, Carrier FEIN, and the Claims Admin Firm Name if different from the Insurance Carrier's.
- Provide the Claims Adjuster's Name and Phone Number.
- If available, fill in the Employer's Name, FEIN, SIC Code, Phone Number, and Address including City, State, and Zip.
- Specify the Employer Location if it's different from the primary address, Nature of Business, Policy Number, Policy Effective and Expiry Dates.
- Indicate whether the employer is Self-Insured.
- Enter the Employee's Name, including Last, First, and Middle Initial, along with their Phone Number, Department, Address, City, State, Zip, Gender, and Marital Status.
- Fill in the Employee’s Occupation Description, NCCI Class Code, SSN, DOB, Date of Hire, Employment Status Code (e.g., Full Time/Regular, Part Time, etc.), and Wages information.
- Provide details about the injury including the Date of Injury, Time of Injury, Time Employee began work on Injury Date, Date Employer Notified of Injury, Body Part Affected Code, Nature of Injury Code, and Cause of Injury Code.
- Explain how the injury or illness occurred, including specifics about the incident, the part of the body affected, and any object or substance that directly caused harm to the employee.
- Enter information about the Treatment including Physician's Name, Hospital or Off-Site Treatment Name and Address, and Initial Treatment details.
- For injuries resulting in death, input Date of Death and details of Dependents including their relationship to the deceased (Widow, Daughter, etc.).
- Indicate whether the injury or illness occurred on the employer’s premises and provide the address where the injury occurred if it was elsewhere.
- Finally, complete the form with the Date Prepared, Preparer's Name & Title, Company Name, and Phone Number at the bottom.
Once the form is fully completed, it must be filed with your insurance carrier immediately. This step is crucial for ensuring timely processing of the claim. Remember, accurate and complete information aids in the smooth progression of the workers' compensation claim, ultimately benefiting all parties involved.
Important Questions on This Form
What is the purpose of the Employer’s First Report of Work Injury or Illness form?
The Employer’s First Report of Work Injury or Illness form is a document mandated by the Tennessee Workers' Compensation Law. Its main purpose is to report any injury or illness that occurs in the workplace, ensuring that the incident is officially documented. This documentation is crucial for the administration of workers' compensation claims, facilitating the process for employees to receive any medical treatment and compensation benefits that may be necessary due to workplace injuries or illnesses.
Who is required to complete this form?
Employers in Tennessee are required to complete and file this form with their insurance carrier immediately after being notified of a work-related injury or illness. It's an essential step for employers to comply with state regulations and to initiate the workers' compensation process for their employees.
What information is needed to fill out the form?
The form requires several pieces of information, including:
- Employer and insurance carrier details, such as names and addresses
- Policy numbers and dates
- Employee's personal and employment information
- Detailed account of the injury or illness, including how it occurred, the nature of the injury or illness, the part of the body affected, and any immediate treatment provided
- Time and date of injury, as well as the time and date the employer was notified
- If applicable, information regarding the death of an employee and dependents
What happens if false information is provided on this form?
Providing false, incomplete, or misleading information on the Employer’s First Report of Work Injury or Illness form is considered a crime under Tennessee law. The penalties for such an act can include imprisonment, fines, and denial of insurance benefits. It is crucial for all information provided on the form to be accurate and truthful to ensure a fair and lawful processing of workers' compensation claims.
Is it required to notify the insurance carrier of all types of injuries or illnesses?
Yes, employers are required to report all types of work-related injuries or illnesses, regardless of their perceived severity. This includes everything from minor injuries that may only require first aid to more serious injuries that result in lost time from work or require significant medical treatment. Reporting all incidents ensures proper documentation and facilitates appropriate responses, including medical care and compensation if needed.
What are the benefits of the Benefit Review System mentioned in the form?
The Benefit Review System is designed to provide assistance to employers and employees navigating the workers' compensation process in Tennessee. A Workers' Compensation Specialist can offer guidance and help resolve any disputes or questions related to workers' compensation claims. The system aims to streamline the claims process and ensure that employees receive the benefits they are entitled to in a timely manner.
What should an employer do if they have questions about completing the form?
If an employer has questions or requires assistance with completing the Employer’s First Report of Work Injury or Illness form, they should contact the Tennessee Department of Labor and Workforce Development. Assistance is available by calling 1-800-332-2667 (TDD), where specialized support for the workers' compensation process can be provided.
Common mistakes
Filling out the Tennessee First Report of Work Injury or Illness form is a critical step in the workers' compensation process. It ensures that employees who are injured or fall ill at work get the support they need. However, mistakes can happen when completing this form. Understanding these common errors can help in avoiding them, ensuring the process moves smoothly for everyone involved.
Here are ten mistakes frequently made on the form:
- Leaving sections blank: Every section of the form should be filled out. If a particular section does not apply, entering "N/A" (for "Not Applicable") ensures that all parts have been considered and addressed.
- Providing incomplete or unclear descriptions of the incident: It's crucial to provide a clear and detailed account of the incident, including what the employee was doing just before the injury, how the injury occurred, and what part of the body was affected. Vague descriptions can delay the processing of the claim.
- Incorrectly listing the date and time of injury: Accuracy in reporting when the injury or illness occurred is essential for the claims process. Mistakes in dates and times can complicate or delay the claim.
- Forgetting to include the employer’s FEIN: The Federal Employer Identification Number (FEIN) is a unique number assigned to each employer. Failing to include it can lead to confusion and processing delays.
- Omitting the insurance carrier or claims administrator information: This information is critical for ensuring that communication about the claim is directed to the right place. Not including it can lead to significant delays.
- Not specifying the nature of the injury, body part affected, and cause of injury codes: These codes help in categorizing the type of injury and its causes clearly. Skipping these details can lead to incorrect processing of the claim.
- Incomplete employee information: Full employee information, including their position, department, and full address, is necessary. This helps in identifying the claimant within the employer's records.
- Misclassifying the employment status: Misunderstanding or incorrectly marking the employee’s employment status (e.g., full-time, part-time, seasonal) can affect eligibility and benefits.
- Incorrect or missing wage information: Accurate wage information is critical for determining compensation rates. Any mistake here can lead to incorrect benefit payments.
- Failing to indicate if full wages were paid for the date of injury: This information helps in determining if compensation adjustments are necessary to cover lost wages from the day of the injury.
Avoiding these mistakes requires careful attention to detail and a thorough understanding of the form. Employers and their representatives should review all information for accuracy before submission. Should questions or uncertainties arise, consulting with the Tennessee Department of Labor and Workforce Development or a workers' compensation specialist can provide clarity and guidance. Ensuring the form is filled out correctly the first time can expedite the claims process, supporting injured workers in their recovery journey.
Documents used along the form
In addition to the Tennessee First Report of Work Injury or Illness form, which is pivotal for initiating a workers' compensation claim process in Tennessee, there are several other documents and forms that frequently accompany or follow the initial filing. These documents play critical roles in various stages of the claims process, supporting both the employer's and employee's responsibilities and rights under the Tennessee Workers' Compensation Law.
- Wage Statement Form: This document is essential for calculating the employee's compensation rate. It details the wages the injured worker earned before the injury, typically encompassing the 52 weeks prior to the incident. It ensures that the compensation is accurately aligned with the employee's earnings.
- Medical Release Form: An authorization form that allows the release of medical information related to the work injury. This form is crucial for the employer’s insurance carrier to obtain medical records that verify the nature and extent of the work-related injury or illness.
- Panel of Physicians Form: This form lists the healthcare providers that an injured worker can choose from for treatment of a work-related injury or illness. It's an integral part of the process as it ensures that workers have access to medical treatment by approved providers.
- Notice of Injury: A written notice that an employee should provide to their employer as soon as possible following an injury. Although not always a formal form, this document is important in the claims process timeline and serves as an official notification of the incident.
- Employer’s Wage Verification Form: Similar to the Wage Statement Form, this document is used for verifying the injured worker's wages. It may be requested by the insurance carrier or the Tennessee Bureau of Workers' Compensation to ensure the accuracy of compensation payments.
- Request for Assistance Form: When disputes arise or when an injured worker needs help navigating the workers' compensation process, this form can be filed with the Tennessee Bureau of Workers' Compensation. It is a plea for intervention, guidance, or resolution from the state's workers' compensation officials.
Understanding the purpose and requirements of each of these documents can significantly streamline the workers' compensation process for employers, employees, and insurers alike. Accurate and timely submission of the appropriate forms not only complies with Tennessee law but also facilitates a smoother and more effective management of workers' compensation claims.
Similar forms
The Workers' Compensation Claim Form, used in various states across the U.S., is similar to the Tennessee First Report form in its primary function to initiate a claim for a work-related injury or illness. Both forms require detailed information about the injured employee, the employer, and specifics of the injury or illness, such as date, time, and how the injury occurred. This ensures timely reporting and processing of workers' compensation claims.
The Occupational Safety and Health Administration (OSHA) Form 300 Log of Work-Related Injuries and Illnesses aligns closely with the Tennessee First Report form. Both documents collect data on work-related injuries and illnesses to comply with legal requirements and support workplace safety. However, the OSHA Form 300 serves more for record-keeping and statistical purposes, while the First Report form is for initiating a compensation claim process.
The Notice of Injury form, which employees must fill out to notify their employers formally about a work-related injury or illness, shares key features with the Tennessee First Report form. Both forms kickstart the documentation and potential claims process following a workplace incident, though the Notice of Information is more focused on the employee's immediate notification to the employer.
The Claim for Benefits form, used in various insurance and workers' compensation scenarios, also parallels the Tennessee First Report form in its purpose. It's designed to formally request compensation or benefits due to injury, illness, or other qualifying events. This form, like the Tennessee First Report, requires comprehensive details about the claimant, the event leading to the claim, and the desired benefits.
The Employer's Report of Occupational Injury or Illness, specific to certain jurisdictions, is akin to the Tennessee First Report in content and intent. Employers utilize this form to report incidents of workplace injuries or illnesses to the relevant regulatory body, detailing the incident and parties involved. It's a critical step for compliance and ensuring employee benefits are dispatched appropriately.
The Accident Report Form, often used for vehicle or general liability claims, shares similarities with the First Report in that it documents specific details about an incident that may lead to a claim. Both forms are integral in the initial stages of investigating and processing a claim, requiring information on the incident's circumstances, those involved, and the extent of injuries or damages.
The Incident Report Form, commonly employed in workplaces for any unusual or unforeseen events, parallels the Tennessee First Report form in its role in early reporting. Both forms collect comprehensive details about the incident, helping in evaluating the event's impact and implementing preventive measures, although the Incident Report is broader in application, covering more than just injuries.
The Disability Claim Form, used for claiming disability benefits from insurance companies or government benefits programs, has pertinent similarities to the Tennessee First Report form regarding its requirement for detailed personal and medical information, the nature of the disability, and the claimant’s employment situation to process a claim.
The Patient's Request for Medical Payment form, used in healthcare insurance claims, relates to the Tennessee First Report form by necessitating detailed information on the patient (or employee), the medical services received, and the circumstances necessitating those services. Both are critical in the financial aspect of covering medical-related expenses.
The Return-to-Work Form serves a slightly different but complementary purpose to the Tennessee First Report form. It's designed for documenting an employee's capability and readiness to return to work following an injury or illness. While the First Report form initiates the claim process immediately after an incident, the Return-to-Work form is pivotal in concluding that process, ensuring a smooth transition back into employment.
Dos and Don'ts
Filling out the Tennessee First Report of Work Injury or Illness form is a critical step in the workers' compensation process. It requires attention to detail and accuracy to ensure the injured worker receives the appropriate benefits and support. Below are five essential dos and don'ts to keep in mind when completing this form:
- Do double-check the form for completeness before submission. Ensuring all sections are filled out accurately can help avoid delays in processing the claim.
- Do provide detailed descriptions of the injury or illness, including the events leading up to it, to give a clear understanding of the circumstances.
- Do report the injury in a timely manner. The form should be filed with your insurance carrier immediately after notice of the injury to comply with Tennessee law.
- Do verify the accuracy of all provided information, especially the employee's personal details and the specifics of the injury or illness.
- Do keep a copy of the completed form for your records. This can be helpful for future reference or if any disputes arise.
- Don't leave sections blank. If a section does not apply, it's better to indicate this with a "N/A" or "Not Applicable" to show that it was not overlooked.
- Don't provide false, incomplete, or misleading information. Remember, it is a crime to knowingly submit incorrect information for workers' compensation transactions.
- Don't ignore instructions or the form's guidelines. Following them closely can help ensure the form is filled out correctly.
- Don't forget to include the preparer’s name, title, and contact information at the end of the form. This can be crucial if clarification or additional information is needed.
- Don't neglect to notify the injured employee about the claim submission. Keeping the employee informed can help manage expectations and support the process.
By adhering to these guidelines, you can help streamline the workers' compensation claim process, ensuring that the injured party receives the necessary assistance and benefits in a timely manner.
Misconceptions
Understanding legal forms is critical, especially when dealing with workplace incidents. The Tennessee First Report form, required under the Tennessee Workers' Compensation Law, is a crucial document in reporting work-related injuries or illnesses. Yet, several misconceptions surround its use and requirements. Let's clear up some of these misunderstandings.
- Only severe injuries should be reported: Every work-related injury or illness, regardless of its severity, must be reported using the Tennessee First Report form. This ensures that even minor incidents are documented, which can be important for ongoing health and safety assessments and potential future claims.
- The form is optional: The use of this form is not optional but a mandatory requirement under the Tennessee Workers' Compensation Law for reporting work injuries or illnesses. Failure to complete and file this document with the insurance carrier immediately after notice of an injury can lead to penalties, including imprisonment, fines, and denial of insurance benefits.
- It’s the employee's responsibility to file the form: It is the employer's responsibility to complete and file the Tennessee First Report of Work Injury or Illness form, not the employee's. This process is crucial for ensuring that the claim is properly documented and processed in a timely manner.
- Falsifying information on the form is a minor issue: Providing false, incomplete, or misleading information on the Tennessee First Report form is a serious offense. It's considered a crime that can lead to severe penalties, including imprisonment, fines, and denial of claims and insurance benefits. Accuracy and honesty when completing this form are absolutely critical.
- The form is only for employees under the Tennessee Workers' Compensation Insurance: Regardless of whether an employer is insured under the Tennessee Workers' Compensation Insurance, they are required to report work-related injuries or illnesses. This document plays a vital role in the administration of workers' compensation claims and helps in streamlining the process for all parties involved.
Clearly, the Tennessee First Report form is pivotal in the landscape of workplace safety and health. Its proper use not only complies with the law but also ensures that employees receive the necessary care and support after a work-related injury or illness. Dispelling the above misconceptions encourages a culture of transparency and responsibility within the workplace.
Key takeaways
Understanding the Tennessee First Report form is crucial for both employers and employees involved in a work-related injury or illness. Here are key takeaways to ensure that the form is filled out correctly and used efficiently:
- Completing the Tennessee First Report form is mandated by the Tennessee Workers' Compensation Law when a work-related injury or illness occurs.
- The form must be filed with the employer’s insurance carrier promptly following the notification of an injury or illness.
- Providing false, incomplete, or misleading information on the form is considered a criminal offense and could lead to penalties including fines, imprisonment, and the denial of insurance benefits.
- Both "Med Only" and "Indemnity Claims" are types of claims that can be reported using this form. It's important to understand the difference to ensure accurate reporting.
- The form requires detailed information, including employer and insurance carrier details, the nature of the employee's business, policy numbers, employee information, and specifics about the injury or illness and how it occurred.
- Details about the injury or illness, such as the date and time it occurred, the body part affected, and a description of the incident, are essential for a thorough report.
- If the injury or illness resulted in or is expected to result in lost time from work, this should be clearly indicated in the appropriate section of the form.
- For cases requiring medical attention, information about the initial treatment and any anticipated major medical treatments or future lost time should be provided.
Remember, the Tennessee First Report form is a key document in the workers' compensation process, ensuring that employees receive appropriate medical care and benefits in the event of work-related injuries or illnesses. Careful and accurate completion of this form is in the best interest of all parties involved.
Create Other Documents
Articles of Organization Tennessee - Stocks, bonds, and similar financial instruments reported must include detailed information for valuation purposes.
Tennessee Ps 0376 - Mandates the disclosure of telemarketing being outsourced, including the third-party company's details.
Tabc Tennessee - Entities must submit accompanying documents such as a non-resident Tennessee license and a copy of the federal basic permit with the Alc 119 form.